ប្រសិនបើម្រាមដៃដែលជាប់គាំងមិនត្រូវបានខូច ឬបែកចេញទេនោះ វាអាចត្រូវបានបិទជាប់នឹងម្រាមដៃរបស់វា ដើម្បីកុំឱ្យវាផ្លាស់ទី ឬហៅថា buddy taping។ (ឈ្នះ SH et al ។ , 2014)
How do healthcare professionals in a chiropractic clinic provide a clinical approach to preventing medical errors for individuals in pain?
មាតិកា
សេចក្តីផ្តើម
Medical errors resulted in 44,000–98,000 hospitalized American deaths annually, and many more caused catastrophic injuries. (Kohn et al., 2000) This was more than the number of people who died annually from AIDS, breast cancer, and auto accidents at the time. According to later research, the actual number of deaths may be closer to 400,000, placing medical errors as the third most common cause of death in the US. Frequently, these mistakes are not the product of medical professionals who are inherently bad; rather, they are the outcome of systemic issues with the health care system, such as inconsistent provider practice patterns, disjointed insurance networks, underutilization or absence of safety protocols, and uncoordinated care. Today’s article looks at the clinical approach to preventing a medical error in a clinical setting. We discuss associated medical providers specializing in various pretreatments to aid individuals suffering from chronic issues. We also guide our patients by allowing them to ask their associated medical providers very important and intricate questions. Dr. Alex Jimenez, DC, only utilizes this information as an educational service. ការមិនទទួលខុសត្រូវ
Defining Medical Errors
Determining what medical error is the most crucial step in any conversation about preventing medical errors. You might assume this is a very easy chore, but that is only until you delve into the vast array of terminology utilized. Many terms are used synonymously (sometimes mistakenly) since some terminology is interchangeable, and occasionally, the meaning of a term depends on the specialty being discussed.
Even though the healthcare sector stated that patient safety and eliminating or reducing medical errors were priorities, Grober and Bohnen noted as recently as 2005 that they had fallen short in one crucial area: determining the definition of “perhaps the most fundamental question… What is a medical error? A medical error is a failure to complete a planned action in a medical setting. (Grober & Bohnen, 2005) However, none of the terms that one would often identify expressly with a medical error—patients, healthcare, or any other element—are mentioned in this description. Despite this, the definition offers a solid framework for further development. As you can see, that specific definition consists of two parts:
An execution error: A failure to complete a planned action as intended.
A planning error: is a technique that, even with perfect execution, does not produce the desired results.
The concepts of faults of execution and planning errors are insufficient if we are to define a medical error adequately. These may occur anywhere, not only at a medical establishment. The component of medical management must be added. This brings up the idea of unfavorable occurrences, known as adverse events. The most common definition of an adverse event is unintentional harm to patients brought about by medical therapy rather than their underlying disease. This definition has gained international acceptance in one way or another. For example, in Australia, the term incidents are defined as in which harm resulted in a person receiving health care. These consist of infections, injury-causing falls, and issues with prescription drugs and medical equipment. Certain unfavorable occurrences might be avoidable.
Common Types of Medical Errors
The only issue with this notion is that not all negative things happen accidentally or intentionally. Because the patient may ultimately benefit, an expected but tolerated adverse event may occur. During chemotherapy, nausea and hair loss are two examples. In this instance, refusing the recommended treatment would be the only sensible approach to prevent the unpleasant consequence. We thus arrive at the concept of preventable and non-preventable adverse occurrences as we further refine our definition. It isn’t easy to categorize a choice to tolerate one impact when it is determined that a favorable effect will occur simultaneously. But purpose alone isn’t necessarily an excuse. (Patient Safety Network, 2016, para.3) Another example of a planned mistake would be a right foot amputation due to a tumor on the left hand, which would be accepting a known and predicted unfavorable event in the hopes of a beneficial consequence where none has ever arisen before. There is no evidence to support the anticipation of a positive outcome.
Medical errors that cause harm to the patient are typically the focus of our research. Nonetheless, medical mistakes can and do occur when a patient is not harmed. The occurrence of near misses could provide invaluable data when planning how to reduce medical errors in a healthcare facility. Still, the frequency of these events compared to the frequency clinicians report them needs to be investigated. Near misses are medical errors that could have caused harm but did not to the patient, even if the patient is doing well. (Martinez et al ។ , 2017) Why would you acknowledge something that could potentially result in legal action? Consider the scenario where a nurse, for whatever reason, had just been looking at photographs of different medications and was about to provide a medication. Maybe something lingers in her memory, and she decides that’s not how a specific medication looks. Upon checking, she found that the incorrect medicines had been administered. After checking all the paperwork, she fixes the mistake and gives the patient the right prescription. Would it be possible to avoid an error in the future if the administration record included photographs of the proper medication? It is easy to forget that there was a mistake and a chance for harm. That fact remains true regardless of whether we were fortunate enough to find it in time or suffer any negative consequences.
Errors of Outcomes & Process
We need complete data to develop solutions that improve patient safety and decrease medical errors. At the very least, when the patient is in a medical facility, everything that can be done to prevent harm and put them in danger should be reported. Many doctors have determined that using the phrases errors and adverse events was more comprehensive and suitable after reviewing mistakes and adverse events in health care and discussing their strengths and weaknesses in 2003. This combined definition would increase data gathering, including mistakes, close calls, near misses, andactive and latent errors. Additionally, the term adverse events includes terms that usually imply patient harm, such as medical injury and iatrogenic injury. The only thing that remains is determining whether a review board is a suitable body to handle the separation of preventable and non-preventable adverse events.
A sentinel event is an occurrence where reporting to the Joint Commission is required. The Joint Commission states that a sentinel event is an unexpected occurrence involving a serious physical or psychological injury. (“Sentinel Events,” 2004, p.35) There isn’t a choice, as it needs to be documented. Most healthcare facilities, however, do keep their records outlining sentinel incidents and what to do in the event of one to guarantee that the Joint Commission standards are met. This is one of those situations when it’s better to be safe than sorry. Since “serious” is a relative concept, there may be some wriggle room when defending a coworker or an employer. On the other hand, reporting a sentinel event incorrectly is better than failing to report a sentinel event. Failing to disclose can have serious consequences, including career termination.
When considering medical errors, people frequently make the mistake of focusing just on prescription errors. Medication errors are undoubtedly frequent and involve many of the same procedural flaws as other medical errors. Breakdowns in communication, mistakes made during prescription or dispensing, and many other things are possible. But we would be gravely misjudging the issue if we assumed that drug errors are the only cause of harm to a patient. One major challenge in classifying the different medical errors is determining whether to classify the error based on the procedure involved or the consequence. It is acceptable to examine those classifications here, given numerous attempts have been made to develop working definitions that incorporate both the process and the outcome, many of which are based on Lucian Leape’s work from the 1990s.
Enhance Your Lifestyle Today- Video
Analyzing & Preventing Medical Errors
Operative and nonoperative were the two main categories of adverse events that Leape and his colleagues distinguished in this study. (Leape et al., 1991) Operative problems included wound infections, surgical failures, non-technical issues, late complications, and technical difficulties. Nonoperative: headings such as medication-related, misdiagnosed, mistreated, procedure-related, fall, fracture, postpartum, anesthesia-related, neonatal, and a catch-all heading of the system were included under this category of adverse occurrences. Leape also classified errors by pointing out the point of process breakdown. He also categorized these into five headings, which include:
ប្រព័ន្ធ
ការសម្តែង
ការព្យាបាលដោយថ្នាំ
រោគវិនិច្ឆ័យ
ការការពារ។
Many process faults fall under more than one topic, yet they all help to pinpoint the exact cause of the issue. If more than one physician was engaged in determining the precise areas that need improvement, then additional questioning might be required.
Technically, a medical error can be made by any staff member at a hospital. It is not limited to medical professionals like physicians and nurses. An administrator may unlatch a door, or a cleaning crew member could leave a chemical within a child’s grasp. What matters more than the identity of the perpetrator of the mistake is the reason behind it. What before it? And how can we make sure that doesn’t occur again? After gathering all the above data and much more, it’s time to figure out how to prevent similar errors. As for sentinel events, the Joint Commission has mandated since 1997 that all of these incidents undergo a procedure called Root Cause Analysis (RCA). However, using this procedure for incidents that need to be reported to outside parties would need to be corrected.
What Is A Root Cause Analysis?
RCAs “captured the details as well as the big picture perspective.” They make evaluating systems easier, analyzing whether remedial action is necessary, and tracking trends. (Williams, 2001) What precisely is an RCA, though? By examining the events that led to the error, an RCA can focus on events and processes rather than reviewing or placing blame on specific people. (AHRQ,2017) This is why it is so crucial. An RCA frequently makes use of a tool called the Five Whys. This is the process of continuously asking yourself “why” after you believe you have determined the cause of an issue.
The reason it’s called the “five whys” is because, while five is an excellent starting point, you should always question why until you identify the underlying cause of the problem. Asking why repeatedly could reveal many process faults at different stages, but you should keep asking why about every aspect of the issue until you run out of other things that could be adjusted to provide a desirable result. However, different tools besides this one can be utilized in a root cause investigation. Numerous others exist. RCAs must be multidisciplinary and consistent and involve all parties involved in the error to avoid misunderstandings or inaccurate reporting of occurrences.
សន្និដ្ឋាន
Medical errors in healthcare institutions are frequent and mostly unreported events that seriously threaten patients’ health. Up to a quarter of a million individuals are thought to pass away each year as a result of medical blunders. These statistics are unacceptable in a time when patient safety is supposedly the top priority, but not much is being done to alter practices. If medical errors are accurately defined and the root cause of the problem is found without assigning blame to specific staff members, this is unnecessary. Essential changes can be made when fundamental causes of system or process faults are correctly identified. A consistent, multidisciplinary approach to root cause analysis that uses frameworks like the five whys to delve down until all issues and defects are revealed is a helpful tool. Although it is now necessary for the wake of sentinel events, the Root Cause Analysis may and should be applied to all mistake causes, including near misses.
Kohn, L. T., Corrigan, J., Donaldson, M. S., & Institute of Medicine (U.S.). Committee on Quality of Health Care in America. (2000). To err is human : building a safer health system. National Academy Press. books.nap.edu/books/0309068371/html/index.html
Leape, L. L., Brennan, T. A., Laird, N., Lawthers, A. G., Localio, A. R., Barnes, B. A., Hebert, L., Newhouse, J. P., Weiler, P. C., & Hiatt, H. (1991). The nature of adverse events in hospitalized patients. Results of the Harvard Medical Practice Study II. N Engl J Med, 324(6), 377-384 ។ doi.org/10.1056/NEJM199102073240605
Martinez, W., Lehmann, L. S., Hu, Y. Y., Desai, S. P., & Shapiro, J. (2017). Processes for Identifying and Reviewing Adverse Events and Near Misses at an Academic Medical Center. Jt Comm J Qual Patient Saf, 43(1), 5-15 ។ doi.org/10.1016/j.jcjq.2016.11.001
អតុល្យភាពនៃបាក់តេរីក្នុងពោះវៀនក៏ត្រូវបានផ្សារភ្ជាប់ទៅនឹងបញ្ហាទល់លាមកផងដែរ។ ការសិក្សាមួយផ្សេងទៀតបានផ្តោតលើឥទ្ធិពលនៃការដើរលឿនធៀបនឹងការធ្វើលំហាត់ប្រាណដែលពង្រឹងសាច់ដុំស្នូលដូចជាបន្ទះក្តារនៅលើសមាសធាតុមីក្រូជីវសាស្ត្រពោះវៀន។ (Morita, E., et al., 2019) លទ្ធផលបានបង្ហាញថាការធ្វើលំហាត់ប្រាណបែប aerobic ដូចជាថាមពល/ការដើរលឿនអាចជួយបង្កើនពោះវៀន បាក់តេរីដែលជាផ្នែកសំខាន់នៃបាក់តេរីពោះវៀនដែលមានសុខភាពល្អ។ ការសិក្សាបានបង្ហាញពីឥទ្ធិពលវិជ្ជមាននៅពេលដែលបុគ្គលចូលរួមក្នុងការដើរយ៉ាងហោចណាស់ ២០ នាទីជារៀងរាល់ថ្ងៃ។ (Morita, E., et al., 2019)
លំហាត់ប្រាណអាចជួយបន្ថយហានិភ័យមហារីកពោះវៀនធំ
សកម្មភាពរាងកាយអាចជាកត្តាការពារដ៏សំខាន់ក្នុងការកាត់បន្ថយជំងឺមហារីកពោះវៀនធំ។ (វិទ្យាស្ថានជាតិមហារីក។ ឆ្នាំ 2023) អ្នកខ្លះប៉ាន់ប្រមាណថាការកាត់បន្ថយហានិភ័យគឺ 50% ហើយការធ្វើលំហាត់ប្រាណថែមទាំងអាចជួយការពារការកើតឡើងវិញបន្ទាប់ពីការធ្វើរោគវិនិច្ឆ័យមហារីកពោះវៀនធំផងដែរ 50% នៅក្នុងការសិក្សាមួយចំនួនចំពោះអ្នកជំងឺដែលមានជំងឺមហារីកពោះវៀនដំណាក់កាលទី II ឬដំណាក់កាលទី III ។ (Schoenberg MH 2016)
អ្នករត់ និងអ្នកដើរខ្លះជួបប្រទះនឹងពោះវៀនធំដែលសកម្មខ្លាំងពេក ដែលបណ្តាលឱ្យរាគទាក់ទងនឹងការធ្វើលំហាត់ប្រាណ ឬលាមករលុង ដែលត្រូវបានគេស្គាល់ថាជាអ្នករត់ប្រណាំង។ រហូតដល់ 50% នៃអត្តពលិកស៊ូទ្រាំបានជួបប្រទះបញ្ហាក្រពះពោះវៀនអំឡុងពេលហាត់ប្រាណខ្លាំង។ (de Oliveira, EP et al., 2014) វិធានការបង្ការដែលអាចត្រូវបានអនុវត្តរួមមាន។
Morita, E., Yokoyama, H., Imai, D., Takeda, R., Ota, A., Kawai, E., Hisada, T., Emoto, M., Suzuki, Y., & Okazaki, K. (2019)។ ការបណ្តុះបណ្តាលលំហាត់ប្រាណតាមបែប Aerobic ជាមួយនឹងការដើរលឿន បង្កើន Bacteroides ពោះវៀនចំពោះស្ត្រីវ័យចំណាស់ដែលមានសុខភាពល្អ។ សារធាតុចិញ្ចឹម, 11(4), 868។ doi.org/10.3390/nu11040868
For individuals looking to improve their fitness health, can a fitness assessment test identify potential areas and help evaluate overall health and physical status?
មាតិកា
ការវាយតម្លៃសម្បទា
A fitness test, also known as a fitness assessment, helps evaluate an individual’s overall and physical health. It comprises a series of exercises to design an appropriate exercise program for general health and fitness. (សមាគមកម្លាំង និងលក្ខខណ្ឌជាតិ។ ឆ្នាំ ២០១៧) Fitness assessment testing benefits include:
Identifying areas that need improvement.
Assisting professionals in understanding what types of exercise are safest and most effective.
Helping measure fitness progress over time.
Allowing for an individualized plan that can help prevent injuries and maintain the body’s overall health.
An assessment can comprise a wide range of tests, including:
Body composition tests.
Cardiovascular stress tests.
Endurance tests.
Range of motion tests.
They are meant to ensure the individual won’t be at risk of injury and provide the trainer with the insights needed to establish clear and effective fitness goals. Individuals who wonder whether fitness testing would benefit them should consult their healthcare provider.
សុខភាពទូទៅ
Before starting a fitness program, it is important to inform the trainer of individual medical history and get the necessary approval from a primary healthcare provider. (Harvard Health Publishing. Harvard Medical School. 2012) Fitness specialists usually use one or more screening tools to help determine individual baseline health.
This may include obtaining vital sign measurements like height and weight, resting heart rate/RHR, and resting blood pressure/RBP. Many trainers will also use a physical activity readiness questionnaire/PAR-Q comprising questions about general health. (បណ្ឌិតសភាវេជ្ជសាស្ត្រកីឡាជាតិ។ ២០២២) Among the questions, individuals may be asked about the medications being taken, any problems with dizziness or pain, or medical conditions that may impair their ability to exercise.
សមាសភាពរាងកាយ
Body composition describes total body weight components, including muscles, bones, and fat. The most common methods for estimating body composition include:
Bioelectrical Impedance Analysis – BIA
During BIA, electrical signals are sent from electrodes through the soles of the feet to the abdomen to estimate body composition. (Doylestown Health. 2024)
These measurements use calipers to estimate the amount of body fat in a fold of skin.
Cardiovascular Endurance
Cardiovascular endurance testing, also known as stress testing, measures how efficiently the heart and lungs work to supply oxygen and energy to the body during physical activity. (UC Davis Health, 2024) The three most common tests used include:
12-minute Run Tests
Twelve-minute run tests are performed on a treadmill, and an individual’s pre-exercise heart and respiration rates are compared with post-exercise heart and respiration rates.
Exercise Stress
Exercise stress testing is performed on a treadmill or stationary bike.
It involves using a heart monitor and blood pressure cuff to measure vital signs during exercise.
VO2 Max Testing
Performed on a treadmill or stationary bike.
V02 max testing uses a breathing device to measure the maximum rate of oxygen consumption during physical activity (UC Davis Health, 2024)
Some trainers will incorporate exercises like sit-ups or push-ups to measure response to specific exercises.
These baseline results can be used later to see if health and fitness levels have improved.
កម្លាំងនិងការស៊ូទ្រាំ
Muscle endurance testing measures the length of time a muscle group can contract and release before it fatigues. Strength testing measures the maximal amount of force a muscle group can exert. (American Council on Exercise, Jiminez C., 2018) The exercises used include:
The push-up test.
Core strength and stability test.
Sometimes, a trainer will use a metronome to measure how long the individual can keep up with the rhythm. The results are then compared to individuals of the same age group and sex to establish a baseline level. Strength and endurance tests are valuable as they help the trainer spot which muscle groups are stronger, vulnerable, and need focused attention. (Heyward, V. H., Gibson, A. L. 2014).
ភាពបត់បែន
Measuring the flexibility of joints is vital in determining whether individuals have postural imbalances, foot instability, or limitations in range of motion. (Pate R, Oria M, Pillsbury L, 2012)
Shoulder Flexibility
Shoulder flexibility testing evaluates the flexibility and mobility of the shoulder joint.
It is performed by using one hand to reach behind the neck, between the shoulders, and the other hand to reach behind the back, toward the shoulders, to measure how far apart the hands are. (Baumgartner TA, PhD, Jackson AS, PhD et al., 2015)
Fitness assessment testing has various benefits. It can help trainers design a personalized workout program, help individuals identify fitness areas that need improvement, measure progress, and add intensity and endurance to their routine, which can help prevent injuries and help maintain overall health. We focus on what works for you and strive to better the body through researched methods and total wellness programs. These natural programs use the body’s ability to achieve improvement goals. Ask a healthcare professional or fitness professional for guidance if you need advice.
Pate R, Oria M, Pillsbury L, (Eds). (2012). Health-related fitness measures for youth: Flexibility. In R. Pate, M. Oria, & L. Pillsbury (Eds.), Fitness Measures and Health Outcomes in Youth. doi.org/10.17226/13483
Can individuals with Ehlers-Danlos syndrome find relief through various non-surgical treatments to reduce joint instability?
មាតិកា
សេចក្តីផ្តើម
The joints and ligaments surrounding the musculoskeletal system allow the upper and lower extremities to stabilize the body and be mobile. The various muscles and soft connective tissues that surround the joints help protect them from injuries. When environmental factors or disorders start to affect the body, many people develop issues that cause overlapping risk profiles, which then affect the stability of the joints. One of the disorders that affect the joints and connective tissue is EDS or Ehlers-Danlos syndrome. This connective tissue disorder can cause the joints in the body to be hypermobile. It can cause joint instability in the upper and lower extremities, thus leaving the individual to be in constant pain. Today’s article focuses on Ehlers-Danlos syndrome and its symptoms and how there are non-surgical ways to manage this connective tissue disorder. We discuss with certified medical providers who consolidate our patients’ information to assess how Ehlers-Danlos syndrome can correlate with other musculoskeletal disorders. We also inform and guide patients on how various non-surgical treatments can help reduce pain-like symptoms and manage Ehlers-Danlos syndrome. We also encourage our patients to ask their associated medical providers many intricate and important questions about incorporating various non-surgical therapies as part of their daily routine to manage the effects of Ehlers-Danlos syndrome. Dr. Jimenez, D.C., includes this information as an academic service. ការមិនទទួលខុសត្រូវ.
What Is Ehlers-Danlos Syndrome?
Do you often feel extremely tired throughout the day, even after a full night of sleep? Do you bruise easily and wonder where these bruises are coming from? Or have you noticed that you have an increased range in your joints? Many of these issues are often correlated with a disorder known as Ehlers-Danlos syndrome or EDS that affects their joints and connective tissue. EDS affects the connective tissues in the body. The connective tissues in the body help provide strength and elasticity to the skin, joints, as well as blood vessel walls, so when a person is dealing with EDS, it can cause a significant disruption to the musculoskeletal system. EDS is largely diagnosed clinically, and many doctors have identified that the gene coding of the collagen and proteins that interact in the body can help determine what type of EDS affects the individual. (Miklovic & Sieg, 2024)
រោគសញ្ញា
When understanding EDS, it is essential to know the complexities of this connective tissue disorder. EDS is classified into numerous types with distinct features and challenges that vary depending on the severity. One of the most common types of EDS is hypermobile Ehlers-Danlos syndrome. This type of EDS is characterized by general joint hypermobility, joint instability, and pain. Some of the symptoms that are associated with hypermobile EDS include subluxation, dislocations, and soft tissue injuries that are common and may occur spontaneously or with minimal trauma. (Hakim, 1993) This can often cause acute pain to the joints in the upper and lower extremities. With its broad range of symptoms and the personal nature of the condition itself, many often don’t realize that joint hypermobility is common in the general population and may present no complications that indicate that it is a connective tissue disorder. (Gensemer et al., 2021) Additionally, hypermobile EDS can lead to spinal deformity due to the hyperextensibility of the skin, joints, and various tissue fragility. The pathophysiology of spinal deformity associated with hypermobile EDS is primarily due to muscle hypotonia and ligament laxity. (Uehara et al., 2023) This causes many people to reduce their quality of life and daily living activities significantly. However, there are ways to manage EDS and its correlating symptoms to reduce joint instability.
Movement Medicine: Chiropractic Care-Video
Ways To Manage EDS
When it comes to looking for ways to manage EDS to reduce pain and joint instability, non-surgical treatments can help address the physical and emotional aspects of the condition. Non-surgical treatments for individuals with EDS commonly focus on optimizing the body’s physical function while improving muscular strength and joint stabilization. (Buryk-Iggers et al., 2022) Many individuals with EDS will try to incorporate pain management techniques and physical therapy anduse braces and assistive devices to reduce the effects of EDS and improve their quality of life.
Non-surgical Treatments For EDS
Various non-surgical treatments like MET (muscle energy technique), electrotherapy, light physical therapy, chiropractic care, and massages can help strengthen while toning the surrounding muscles around the joints, provide sufficient pain relief, and limit long-term dependence on medications. (Broida et al., 2021) Additionally, individuals dealing with EDS aim to strengthen the affected muscles, stabilize the joints, and improve proprioception. Non-surgical treatments allow the individual to have a customized treatment plan for the severity of EDS symptoms and help reduce the pain associated with the condition. Many individuals, when going through their treatment plan consecutively to manage their EDS and reduce the pain-like symptoms, will notice improvement in symptomatic discomfort. (Khokhar et al., 2023) This means that non-surgical treatments allow individuals to be more mindful of their bodies and reduce the pain-like effects of EDS, thus allowing many individuals with EDS to lead fuller, more comfortable lives without feeling pain and discomfort.
ឯកសារយោង
Broida, S. E., Sweeney, A. P., Gottschalk, M. B., & Wagner, E. R. (2021). Management of shoulder instability in hypermobility-type Ehlers-Danlos syndrome. JSES Rev Rep Tech, 1(3), 155-164 ។ doi.org/10.1016/j.xrrt.2021.03.002
Buryk-Iggers, S., Mittal, N., Santa Mina, D., Adams, S. C., Englesakis, M., Rachinsky, M., Lopez-Hernandez, L., Hussey, L., McGillis, L., McLean, L., Laflamme, C., Rozenberg, D., & Clarke, H. (2022). Exercise and Rehabilitation in People With Ehlers-Danlos Syndrome: A Systematic Review. Arch Rehabil Res Clin Transl, 4(2), 100189 ។ doi.org/10.1016/j.arrct.2022.100189
Gensemer, C., Burks, R., Kautz, S., Judge, D. P., Lavallee, M., & Norris, R. A. (2021). Hypermobile Ehlers-Danlos syndromes: Complex phenotypes, challenging diagnoses, and poorly understood causes. Dev Dyn, 250(3), 318-344 ។ doi.org/10.1002/dvdy.220
Hakim, A. (1993). Hypermobile Ehlers-Danlos Syndrome. In M. P. Adam, J. Feldman, G. M. Mirzaa, R. A. Pagon, S. E. Wallace, L. J. H. Bean, K. W. Gripp, & A. Amemiya (Eds.), GeneReviews((R)). www.ncbi.nlm.nih.gov/pubmed/20301456
Khokhar, D., Powers, B., Yamani, M., & Edwards, M. A. (2023). The Benefits of Osteopathic Manipulative Treatment on a Patient With Ehlers-Danlos Syndrome. Cureus, 15(5), e38698 ។ doi.org/10.7759/cureus.38698
Can understanding the body’s hinge joints and how they operate help with mobility and flexibility problems and manage conditions for individuals with difficulty fully bending or extending their fingers, toes, elbows, ankles, or knees?
មាតិកា
Hinge Joints
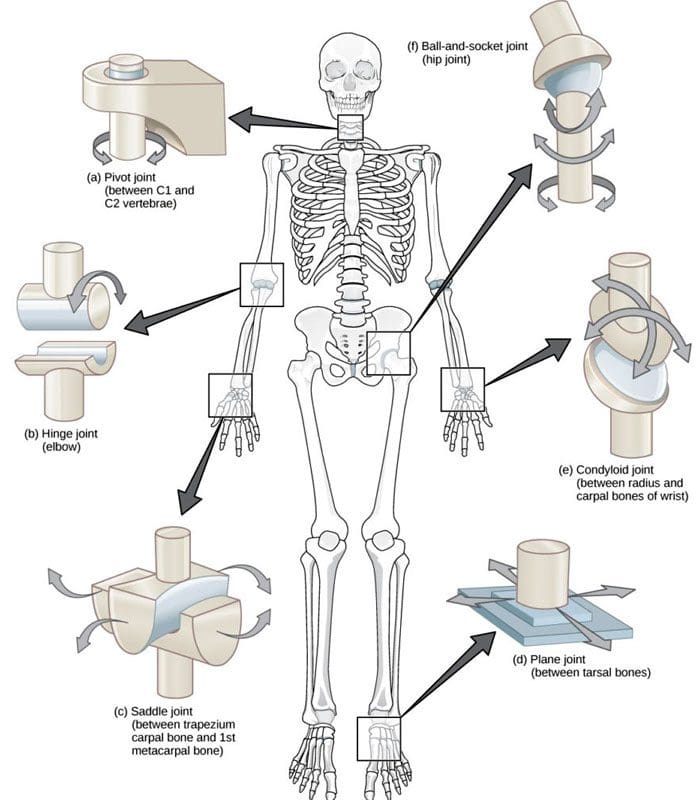
A joint forms where one bone connects to another, allowing motion. Different types of joints differ in structure and movement depending on their location. These include hinge, ball and socket, planar, pivot, saddle, and ellipsoid joints. (Boundless. General Biology, N.D.) Hinge joints are synovial joints that move through one plane of motion: flexion and extension. Hinge joints are found in the fingers, elbows, knees, ankles, and toes and control movement for various functions. Injuries, osteoarthritis, and autoimmune conditions can affect hinge joints. Rest, medication, ice, and physical therapy can help alleviate pain, improve strength and range of motion, and help manage conditions.
កាយវិភាគសាស្ត្រ
A joint is formed by the joining of two or more bones. The human body has three main classifications of joints, categorized by the degree to which they can move. These include: (Boundless. General Biology, N.D.)
Synarthroses
These are fixed, immovable joints.
Formed by two or more bones.
Amphiarthroses
Also known as cartilaginous joints.
A fibrocartilage disc separates the bones that form the joints.
These movable joints allow for a slight degree of movement.
Diarthroses
Also known as synovial joints.
These are the most common freely mobile joints that allow movement in multiple directions.
The bones that form the joints are lined with articular cartilage and enclosed in a joint capsule filled with synovial fluid that allows for smooth motion.
Synovial joints are classified into different types depending on differences in structure and the number of motion planes they allow. A hinge joint is a synovial joint that allows movement in one plane of motion, similar to a door hinge that moves forward and backward. Within the joint, the end of one bone is typically convex/pointed outward, with the other concave/rounded inward to allow the ends to fit smoothly. Because hinge joints only move through one plane of movement, they tend to be more stable than other synovial joints. (Boundless. General Biology, N.D.) Hinge joints include:
The finger and toe joints – allow the fingers and toes to bend and extend.
The elbow joint – allows the elbow to bend and extend.
The knee joint – allows the knee to bend and extend.
The talocrural joint of the ankle – allows the ankle to move up/dorsiflexion and down/plantarflexion.
Hinge joints allow the limbs, fingers, and toes to extend away and bend toward the body. This movement is essential for activities of daily living, such as showering, getting dressed, eating, walking, standing up, and sitting down.
លក្ខខណ្ឌ
Osteoarthritis and inflammatory forms of arthritis can affect any joint (មូលនិធិជំងឺរលាកសន្លាក់។ អិន) Autoimmune inflammatory forms of arthritis, including rheumatoid and psoriatic arthritis, can cause the body to attack its own joints. These commonly affect the knees and fingers, resulting in swelling, stiffness, and pain. (Kamata, M., Tada, Y. 2020) Gout is an inflammatory form of arthritis that develops from elevated levels of uric acid in the blood and most commonly affects the hinge joint of the big toe. Other conditions that affect hinge joints include:
Injuries to the cartilage within the joints or ligaments that stabilize the outside of the joints.
Ligament sprains or tears can result from jammed fingers or toes, rolled ankles, twisting injuries, and direct impact on the knee.
These injuries can also affect the meniscus, the tough cartilage within the knee joint that helps cushion and absorb shock.
ការស្តារឡើងវិញ
Conditions that affect hinge joints often cause inflammation and swelling, resulting in pain and limited mobility.
After an injury or during an inflammatory condition flare-up, limiting active movement and resting the affected joint can reduce increased stress and ការឈឺចាប់.
Applying ice can decrease inflammation and swelling.
Once the pain and swelling start to subside, physical and/or occupational therapy can help rehabilitate the affected areas.
A therapist will provide stretches and exercises to help improve the joint range of motion and strengthen the supporting muscles.
For individuals experiencing hinge joint pain from an autoimmune condition, biologic medications to decrease the body’s autoimmune activity are administered through infusions delivered every several weeks or months. (Kamata, M., Tada, Y. 2020)
Cortisone injections may also be used to decrease inflammation.
Kamata, M., & Tada, Y. (2020). Efficacy and Safety of Biologics for Psoriasis and Psoriatic Arthritis and Their Impact on Comorbidities: A Literature Review. International journal of molecular sciences, 21(5), 1690. doi.org/10.3390/ijms21051690
For individuals dealing with sciatica, can non-surgical treatments like chiropractic care and acupuncture reduce pain and restore function?
មាតិកា
សេចក្តីផ្តើម
The human body is a complex machine that allows the host to be mobile and stable when resting. With various muscle groups in the upper and lower body portions, the surrounding muscles, tendons, nerves, and ligaments serve a purpose for the body as they all have specific jobs in keeping the host functional. However, many individuals have developed various habits that cause strenuous activities that cause repetitive motions to their muscles and nerves and affect their musculoskeletal system. One of the nerves that many individuals have been dealing with pain is the sciatic nerve, which causes many issues in the lower body extremities and, when not treated right away, leads to pain and disability. Luckily, many individuals have sought non-surgical treatments to reduce sciatica and restore body function to the individual. Today’s article focuses on understanding sciatica and how non-surgical therapies like chiropractic care and acupuncture can help reduce the sciatic pain-like effects that are causing overlapping risk profiles in the lower body extremities. We discuss with certified medical providers who consolidate with our patients’ information to assess how sciatica is often correlated with environmental factors that cause dysfunction in the body. We also inform and guide patients on how various non-surgical treatments can help reduce sciatica and its correlating symptoms. We also encourage our patients to ask their associated medical providers many intricate and important questions about incorporating various non-surgical therapies as part of their daily routine to reduce the chances and effects of sciatica from returning. Dr. Jimenez, D.C., includes this information as an academic service. ការមិនទទួលខុសត្រូវ.
ការយល់ដឹងអំពី Sciatica
Do you often feel radiating pain that travels down one or both legs when sitting down for a long period? How often have you experienced tingling sensations that cause you to shake your leg to reduce the effect? Or have you noticed that stretching your legs causes temporary relief? While these overlapping pain symptoms can affect the lower extremities, many individuals may think it is low back pain, but in actuality, it is sciatica. Sciatica is a common musculoskeletal condition that affects many people worldwide by causing pain to the sciatic nerve and radiating down to the legs. The sciatic nerve is pivotal in providing direct and indirect motor function to the leg muscles. (Davis et al ។ , 2024) When the sciatic nerve is compressed, many people state that the pain can vary in intensity, accompanied by symptoms like tingling, numbness, and muscle weakness that can affect a person’s ability to walk and function.
However, some of the root causes that lead to the development of sciatica can play into the factor that causes the pain in the lower extremities. Several inherent and environmental factors are often associated with sciatica, causing lumbar nerve root compression on the sciatic nerve. Factors like poor health status, physical stress, and occupational work are correlated with the development of sciatica and can impact a person’s routine. (Gimenez-Campos et al., 2022) Additionally, some of the root causes of sciatica can include musculoskeletal conditions like herniated discs, bone spurs, or spinal stenosis, which can correlate with these inherent and environmental factors that can reduce many individuals’ motility and life quality. (Zhou និងអ្នកផ្សេងទៀត, 2021) This causes many individuals to seek out treatments to relieve sciatica pain and its correlating symptoms. While the pain caused by sciatica can vary, many individuals often seek non-surgical treatments to alleviate their discomfort and pain from sciatica. This allows them to incorporate effective solutions to managing sciatica.
Beyond Adjustments: Chiropractic & Integrative Healthcare- Video
ការថែទាំតាមបែប Chiropractic សម្រាប់ Sciatica
When it comes to seeking non-surgical treatments to reduce sciatica, non-surgical treatments can reduce the pain-like effects while helping restore body function and mobility. At the same time, non-surgical treatments are customized to the individual’s pain and can be incorporated into a person’s routine. Some non-surgical treatments like chiropractic care are excellent in reducing sciatica and its associated pain symptoms. Chiropractic care is a form of non-surgical therapy that focuses on restoring the body’s spinal movement while improving body function. Chiropractic care utilizes mechanical and manual techniques for sciatica to realign the spine and help the body heal naturally without surgery or medication. Chiropractic care can help decrease intradiscal pressure, increase intervertebral disc space height, and improve the range of motion in the lower extremities. (Gudavalli et al., 2016) When dealing with sciatica, chiropractic care can alleviate the unnecessary pressure on the sciatic nerve and help reduce the risk of reoccurrence through consecutive treatments.
The Effects of Chiropractic Care For Sciatica
Some of the effects of chiropractic care for reducing sciatica can provide insight to the person as chiropractors work with associated medical providers to devise a personalized plan to relieve the pain-like symptoms. Many people who utilize chiropractic care to reduce the effects of sciatica can incorporate physical therapy to strengthen the weak muscles that surround the lower back, stretch to improve flexibility and be more mindful of what factors are causing sciatic pain in their lower extremities. Chiropractic care may guide many people on proper poster ergonomics, and various exercises to reduce the chances of sciatica returning while offering positive effects to the lower body.
Acupuncture For Sciatica
Another form of non-surgical treatment that can help reduce the pain-like effects of sciatica is acupuncture. As a key component in traditional Chinese medicine, acupuncture therapy involves professionals placing thin, solid needles at specific points on the body. នៅពេលដែលវាមកដល់ reducing sciatica, acupuncture therapy can exert analgesic effects on the body’s acupoints, regulate the microglia, and modulate certain receptors along the pain pathway to the nervous system. (Zhang et al ។ , 2023) Acupuncture therapy focuses on restoring the body’s natural energy flow or Qi to promote healing.
The Effects of Acupuncture For Sciatica
Regarding the effects of acupuncture therapy on reducing sciatica, acupuncture therapy can help reduce the pain signals that sciatica produces by changing the brain signal and rerouting the corresponding motor or sensory disturbance of the affected area. (Yu et al ។ , 2022 ។) Additionally, acupuncture therapy can help provide pain relief by releasing endorphins, the body’s natural pain reliever, to the specific acupoint that correlates with the sciatic nerve, reducing inflammation around the sciatic nerve, thus alleviating pressure and pain and helping improve nerve function. Both chiropractic care and acupuncture offer valuable non-surgical treatment options that can provide aid in the healing process and reduce pain caused by sciatica. When many people are dealing with sciatica and looking for numerous solutions to reduce the pain-like effects, these two non-surgical treatments can help many people address the underlying causes of sciatica, enhance the body’s natural healing process, and help provide significant relief from the pain.
Gimenez-Campos, M. S., Pimenta-Fermisson-Ramos, P., Diaz-Cambronero, J. I., Carbonell-Sanchis, R., Lopez-Briz, E., & Ruiz-Garcia, V. (2022). A systematic review and meta-analysis of the effectiveness and adverse events of gabapentin and pregabalin for sciatica pain. Aten Primaria, 54(1), 102144 ។ doi.org/10.1016/j.aprim.2021.102144
Gudavalli, M. R., Olding, K., Joachim, G., & Cox, J. M. (2016). Chiropractic Distraction Spinal Manipulation on Postsurgical Continued Low Back and Radicular Pain Patients: A Retrospective Case Series. J Chiropr Med, 15(2), 121-128 ។ doi.org/10.1016/j.jcm.2016.04.004
What are the healing times of common sports injuries for athletes and individuals who engage in recreational sports activities?
A young, happy sportswoman is getting tens-electrotherapy treatments at a medical clinic.
មាតិកា
Healing Times for Sports Injuries
Healing time from sports injuries depends on various factors, such as the location and extent of the injury and the health of the skin, joints, tendons, muscles, and bones. It is also important to take the time to recuperate or not rush back into physical sports activities before the bones or tissues have fully healed. To prevent re-injury, ensure the doctor clears health before returning to sports or strenuous physical activity.
According to CDC research, an average of 8.6 million sports and recreation-related injuries occur annually. (Sheu, Y., Chen, L. H., and Hedegaard, H. 2016) However, most sports injuries are superficial or caused by low-grade strains or sprains; at least 20% of injuries result from bone fractures or more serious injuries. Bone fractures take longer than sprains or strains, and complete tendon or muscle ruptures can take months before one can fully return to activities. Individuals in decent physical shape with no underlying illness or impairment, here is what they can expect when recovering from the following sports injuries:
ការបាក់ឆ្អឹង
In sports, the highest rate of bone fractures occurs with football and contact sports. Most are centered around the lower extremities but can involve the neck and shoulder blades, arms, and ribs.
Simple Fractures
Depends on the individual’s age, health, type, and location.
Generally, takes at least six weeks to heal.
Compound Fractures
In this case, a bone is broken in several places.
It may require surgery to stabilize the bone.
Healing time can take up to eight months.
Fractured Clavicle/Collarbone
It may require the immobilization of the shoulder and upper arm.
It can take five to ten weeks to heal fully.
Fractured fingers or toes can heal in three to five weeks.
Fractured Ribs
Part of the treatment plan includes breathing exercises.
Painkillers may be needed short term.
Usually, it takes around six weeks to heal.
Neck Fractures
It may involve any one of the seven neck vertebrae.
A neck brace or a halo device that is screwed into the skull for stability may be used.
A sprain is the stretching or tearing of ligaments or the tough bands of fibrous tissue that connect two bones at a joint.
A សំពាធ is the overstretching or tearing of muscles or សរសៃពួរ.
Sprained Ankles
It can heal in five days if there are no complications.
Severe sprains involving torn or ruptured tendons can take three to six weeks to heal.
Calf Strains
Classified as grade 1 – a mild strain can heal in two weeks.
A grade 3 – severe strain may require three months or more to heal completely.
The use of calf suppression sleeves can expedite the recovery of strains and sprains in the lower leg.
Acute Neck Strain
A tackle, impact, fall, quick shifting, or whipping motion can cause a whiplash injury.
Healing time can take a couple of weeks to six weeks.
របួសផ្សេងៗ
ទឹកភ្នែក ACL
Involving the anterior cruciate ligament.
Usually, it requires months of recuperation and rehabilitation, depending on several factors, including the type of sports activity.
Full recovery from surgery takes six to 12 months.
Without surgery, there is no specific timeline for rehabilitation.
Achilles Tendon Ruptures
It is a serious injury.
These occur when the tendon is either partially or completely torn.
Individuals will more than likely require surgery.
Recovery time is four to six months.
ការកាត់បន្ថយនិងការរហែក
Depends on the depth and location of the injury.
It can take anywhere from a week to a month to heal.
If there are no accompanying injuries, stitches can be removed within two to three weeks.
If a deep cut requires stitches, more time is necessary.
Mild Contusions/Bruises
Are caused by a trauma to the skin, causing blood vessels to break.
In most cases, a contusion will take five to seven days to heal.
Shoulder Separations
When treated properly, it usually takes around two weeks of rest and recovery before the patient returns to activity.
Multidisciplinary Treatment
After the initial inflammation and swelling have subsided, a doctor will recommend a treatment plan that usually involves physical therapy, self-performed physical rehabilitation, or supervision by a physical therapist or team. Fortunately, athletes and individuals who regularly exercise tend to have a faster healing time because they are in top physical shape, and their cardiovascular system provides a stronger blood supply that speeds up the healing process. At El Paso’s Chiropractic Rehabilitation Clinic & Integrated Medicine Center, we passionately focus on treating patients’ injuries and chronic pain syndromes. We focus on improving ability through flexibility, mobility, and agility programs tailored to the individual. We use in-person and virtual health coaching and comprehensive care plans to ensure every patient’s personalized care and wellness outcomes.
Our providers use an integrated approach to create personalized care plans that include Functional Medicine, Acupuncture, Electro-Acupuncture, and Sports Medicine principles. Our goal is to relieve pain naturally by restoring health and function to the body.
If the chiropractor feels the individual needs other treatment, they will be referred to a clinic or physician best suited for them. Dr. Jimenez has teamed up with the top surgeons, clinical specialists, medical researchers, and premier rehabilitation providers to provide the top clinical treatments for our community. Providing highly noninvasive protocols is our priority, and our personalized patient-based clinical insight is what we provide.
Sheu, Y., Chen, L. H., & Hedegaard, H. (2016). Sports- and Recreation-related Injury Episodes in the United States, 2011-2014. National health statistics reports, (99), 1–12.
For individuals experiencing pelvic pain, it could be a disorder of the pudendal nerve known as pudendal neuropathy or neuralgia that leads to chronic pain. The condition can be caused by pudendal nerve entrapment, where the nerve becomes compressed or damaged. Can knowing the symptoms help healthcare providers correctly diagnose the condition and develop an effective treatment plan?
មាតិកា
Pudendal Neuropathy
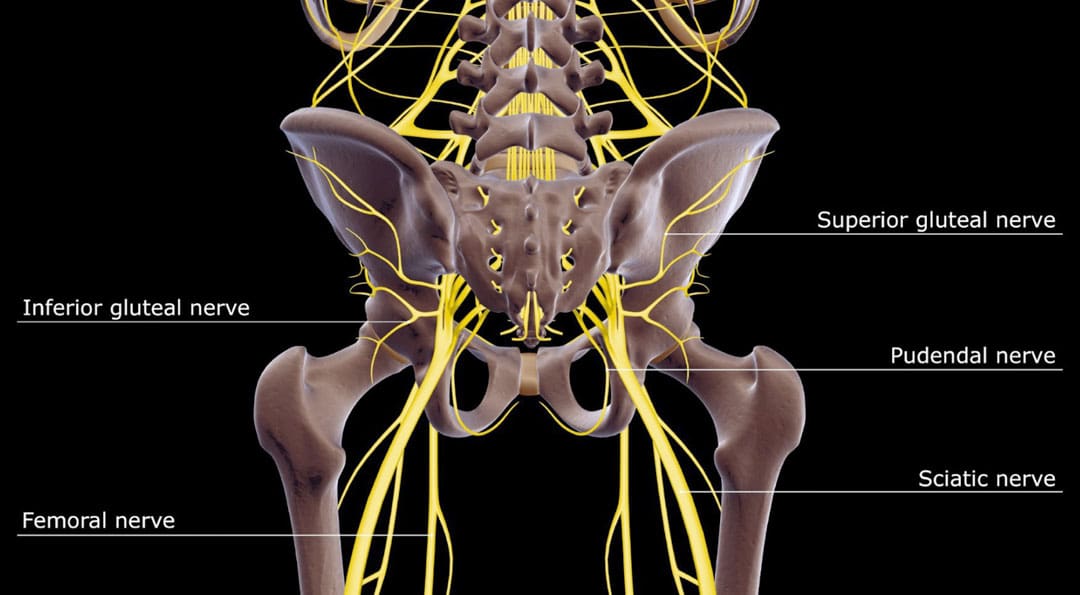
The pudendal nerve is the main nerve that serves the perineum, which is the area between the anus and the genitalia – the scrotum in men and the vulva in women. The pudendal nerve runs through the gluteus muscles/buttocks and into the perineum. It carries sensory information from the external genitalia and the skin around the anus and perineum and transmits motor/movement signals to various pelvic muscles. (Origoni, M. et al., 2014) Pudendal neuralgia, also referred to as pudendal neuropathy, is a disorder of the pudendal nerve that can lead to chronic pelvic pain.
មូលហេតុ
Chronic pelvic pain from pudendal neuropathy can be caused by any of the following (Kaur J. et al., 2024)
Excessive sitting on hard surfaces, chairs, bicycle seats, etc. Bicyclists tend to develop pudendal nerve entrapment.
Trauma to the buttocks or pelvis.
ការសម្រាលកូន។
ជំងឺសរសៃប្រសាទជំងឺទឹកនោមផ្អែម។
Bony formations that push against the pudendal nerve.
Thickening of ligaments around the pudendal nerve.
មានរោគសញ្ញា
Pudendal nerve pain can be described as stabbing, cramping, burning, numbness, or pins and needles and can present (Kaur J. et al., 2024)
In the perineum.
In the anal region.
In men, pain in the scrotum or penis.
In women, pain in the labia or vulva.
អំឡុងពេលរួមភេទ។
When urinating.
During a bowel movement.
When sitting and goes away after standing up.
Because the symptoms are often hard to distinguish, pudendal neuropathy can often be hard to differentiate from other types of chronic pelvic pain.
Cyclist’s Syndrome
Prolonged sitting on a bicycle seat can cause pelvic nerve compression, which can lead to chronic pelvic pain. The frequency of pudendal neuropathy (chronic pelvic pain caused by entrapment or compression of the pudendal nerve) is often referred to as Cyclist’s Syndrome. Sitting on certain bicycle seats for long periods places significant pressure on the pudendal nerve. The pressure can cause swelling around the nerve, which causes pain and, over time, can lead to nerve trauma. Nerve compression and swelling can cause pain described as burning, stinging, or pins and needles. (Durante, J. A., and Macintyre, I. G. 2010) For individuals with pudendal neuropathy caused by bicycling, symptoms can appear after prolonged biking and sometimes months or years later.
Take breaks at least 20–30 seconds after each 20 minutes of riding.
While riding, change positions frequently.
Stand up to pedal periodically.
Take time off between riding sessions and races to rest and relax the pelvic nerves. 3–10 day breaks can help in recovery. (Durante, J. A., and Macintyre, I. G. 2010)
If pelvic pain symptoms are barely starting to develop, rest and see a healthcare provider or specialist for an examination.
កៅអី
Use a soft, wide seat with a short nose.
Have the seat level or tilted slightly forward.
Seats with cutout holes place more pressure on the perineum.
If numbness or pain is present, try a seat without holes.
ការបំពាក់កង់
Adjust the seat height so the knee is slightly bent at the bottom of the pedal stroke.
The body’s weight should rest on the sitting bones/ischial tuberosities.
Keeping the handlebar height below the seat can reduce pressure.
The Triathlon bike’s extreme-forward position should be avoided.
A more upright posture is better.
Mountain bikes have been associated with an increased risk of erectile dysfunction than road bikes.
ខ្លី
Wear padded bike shorts.
ការព្យាបាល
A healthcare provider may use a combination of treatments.
The neuropathy can be treated with rest if the cause is excessive sitting or cycling.
Injury Medical Chiropractic and Functional Medicine Clinic care plans and clinical services are specialized and focused on injuries and the complete recovery process. Our areas of practice include Wellness and nutrition, Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, severe sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, and Functional Medicine Treatments. If the individual requires other treatment, they will be referred to a clinic or physician best suited for their condition, as Dr. Jimenez has teamed with the top surgeons, clinical specialists, medical researchers, therapists, trainers, and premiere rehabilitation providers.
ការមានផ្ទៃពោះនិង Sciatica
ឯកសារយោង
Origoni, M., Leone Roberti Maggiore, U., Salvatore, S., & Candiani, M. (2014). Neurobiological mechanisms of pelvic pain. BioMed research international, 2014, 903848. doi.org/10.1155/2014/903848
Durante, J. A., & Macintyre, I. G. (2010). Pudendal nerve entrapment in an Ironman athlete: a case report. The Journal of the Canadian Chiropractic Association, 54(4), 276–281.
Chiaramonte, R., Pavone, P., & Vecchio, M. (2021). Diagnosis, Rehabilitation and Preventive Strategies for Pudendal Neuropathy in Cyclists, A Systematic Review. Journal of functional morphology and kinesiology, 6(2), 42. doi.org/10.3390/jfmk6020042
For individuals who have exhausted all other treatment options for low back pain and nerve root compression, can laser spine surgery help alleviate nerve compression and provide long-lasting pain relief?
មាតិកា
Laser Spine Surgery
Laser spine surgery is a minimally invasive surgical procedure that uses a laser to cut through and remove spinal structures that are compressing nerves and causing intense pain. The minimally invasive procedure often results in less pain, tissue damage, and faster recovery than more extensive surgeries.
របៀបដែលវាធ្វើការ
Minimally invasive procedures result in less scarring and damage to surrounding structures, often reducing pain symptoms and a shorter recovery time. (Stern, J. 2009) Small incisions are made to access spinal column structures. With open-back surgery, a large incision is made down the back to access the spine. The surgery differs from other surgeries in that a laser beam, rather than other surgical instruments, is used to cut structures in the spine. However, the initial incision through the skin is made with a surgical scalpel. Laser is an acronym for Light Amplification Stimulated by Emission of Radiation. A laser can generate intense heat to cut through soft tissues, especially those with a high water content, like spinal column discs. (Stern, J. 2009) For many spine surgeries, the laser cannot be used to cut through bone as it generates instant sparks that can damage surrounding structures. Rather, laser spine surgery is primarily used to perform a discectomy, which is a surgical technique that removes a portion of a bulging or herniated disc that is pushing against the surrounding nerve roots, causing nerve compression and sciatic pain. (Stern, J. 2009)
Surgical Risks
Laser spine surgery may help resolve the cause of nerve root compression, but there is an increased risk of damage to nearby structures. Associated risks include: (Brouwer, P. A. et al., 2015)
ការឆ្លង
ហូរឈាម
កំណកឈាម
Remaining symptoms
Returning symptoms
Further nerve damage
Damage to the membrane around the spinal cord.
ត្រូវការការវះកាត់បន្ថែម
A laser beam is not precise like other surgical tools and requires practiced mastery and control to avoid damage to the spinal cord and nerve roots. (Stern, J. 2009) Because lasers cannot cut through bone, other surgical instruments are often used around corners and at different angles because they are more efficient and allow greater accuracy. (Atlantic Brain and Spine, 2022)
គោលបំណង
Laser spine surgery is performed to remove structures that are causing nerve root compression. Nerve root compression is associated with the following conditions (គ្លីនិក Cleveland ។ ២០២៣)
បញ្ឆេះឌីស
ឌីសសឺរ
Sciatica
ខួរឆ្អឹងខ្នង
ដុំសាច់ខួរឆ្អឹងខ្នង
Nerve roots that are injured or damaged and constantly send chronic pain signals can be ablated with laser surgery, known as nerve ablation. The laser burns and destroys the nerve fibers. (Stern, J. 2009) Because laser spine surgery is limited in treating certain spinal disorders, most minimally invasive spine procedures do not use a laser. (Atlantic Brain and Spine. 2022)
ការរៀបចំ
The surgical team will provide more detailed instructions on what to do in the days and hours before surgery. To promote optimal healing and a smooth recovery, it is recommended that the patient stay active, eat a healthy diet, and stop smoking prior to the operation. Individuals may need to stop taking certain medications to prevent excess bleeding or interaction with anesthesia during the operation. Inform the healthcare provider about all prescriptions, over-the-counter drugs, and supplements being taken.
Laser spine surgery is an outpatient procedure at a hospital or outpatient surgical center. The patient will likely go home on the same day of the operation. (គ្លីនិក Cleveland ។ ២០២៣) Patients cannot drive to or from the hospital before or after their surgery, so arrange for family or friends to provide transportation. Minimizing stress and prioritizing healthy mental and emotional well-being is important to lowering inflammation and aiding recovery. The healthier the patient goes into surgery, the easier the recovery and rehabilitation will be.
ការរំពឹងទុក
The surgery will be decided by the patient and healthcare provider and scheduled at a hospital or outpatient surgical center. Arrange for a friend or family member to drive to the surgery and home.
មុនពេលវះកាត់
The patient will be taken to a pre-operative room and asked to change into a gown.
The patient will undergo a brief physical examination and answer questions about medical history.
The patient lies on a hospital bed, and a nurse inserts an IV to deliver medication and fluids.
The surgical team will use the hospital bed to transport the patient in and out of the operating room.
The surgical team will assist the patient in getting onto the operating table, and the patient will be administered anesthesia.
The patient may receive ការប្រើថ្នាំសន្លប់ទូទៅ, which will cause the patient to sleep for the surgery, or regional anesthesia, injected into the spine to numb the affected area. (គ្លីនិក Cleveland ។ ២០២៣)
The surgical team will sterilize the skin where the incision will be made.
An antiseptic solution will be used to kill bacteria and prevent the risk of infection.
Once sanitized, the body will be covered with sterilized linens to keep the surgical site clean.
ក្នុងអំឡុងពេលវះកាត់
For a discectomy, the surgeon will make a small incision less than one inch in length with a scalpel along the spine to access the nerve roots.
A surgical tool called an endoscope is a camera inserted into the incision to view the spine. (Brouwer, P. A. et al., 2015)
Once the problematic disc portion causing the compression is located, the laser is inserted to cut through it.
The cut disc portion is removed, and the incision site is sutured.
បន្ទាប់ពីការវះកាត់
After surgery, the patient is brought to a recovery room, where vital signs are monitored as the effects of the anesthesia wear off.
Once stabilized, the patient can usually go home one or two hours after the operation.
The surgeon will determine when the individual is clear to resume driving.
ការងើបឡើងវិញ
Following a discectomy, the individual can return to work within a few days to a few weeks, depending on the severity, but it can take up to three months to return to normal activities. Length of recovery can range from two to four weeks or less to resume a sedentary job or eight to 12 weeks for a more physically demanding job that requires heavy lifting. (University of Wisconsin School of Medicine and Public Health, 2021) During the first two weeks, the patient will be given restrictions to facilitate the spine’s healing until it becomes more stable. Restrictions can include: (University of Wisconsin School of Medicine and Public Health, 2021)
No bending, twisting, or lifting.
No strenuous physical activity, including exercise, housework, yard work, and sex.
No alcohol in the initial stage of recovery or while taking narcotic pain medications.
No driving or operating a motor vehicle until discussed with the surgeon.
The healthcare provider may recommend ការព្យាបាលដោយរាងកាយ to relax, strengthen, and maintain musculoskeletal health. Physical therapy may be two to three times weekly for four to six weeks.
ដំណើរការ
Optimal recovery recommendations include:
Getting enough sleep, at least seven to eight hours.
Maintaining a positive attitude and learning how to cope and manage stress.
Maintaining body hydration.
Following the exercise program as prescribed by the physical therapist.
Practicing healthy posture with sitting, standing, walking, and sleeping.
Staying active and limiting the amount of time spent sitting. Try to get up and walk every one to two hours during the day to stay active and prevent blood clots. Gradually increase the amount of time or distance as recovery progresses.
Do not push to do too much too soon. Overexertion can increase pain and delay recovery.
Learning correct lifting techniques to utilize the core and leg muscles to prevent increased pressure on the spine.
Discuss treatment options for managing symptoms with a healthcare provider or specialist to determine if laser spine surgery is appropriate. Injury Medical Chiropractic and Functional Medicine Clinic care plans and clinical services are specialized and focused on injuries and the complete recovery process. Dr. Jimenez has teamed with the top surgeons, clinical specialists, medical researchers, therapists, trainers, and premiere rehabilitation providers. We focus on restoring normal body functions after trauma and soft tissue injuries using Specialized Chiropractic Protocols, Wellness Programs, Functional and integrative Nutrition, Agility and mobility Fitness Training, and Rehabilitation Systems for all ages. Our areas of practice include Wellness & Nutrition, Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Functional Medicine Treatments, and in-scope care protocols.
Brouwer, P. A., Brand, R., van den Akker-van Marle, M. E., Jacobs, W. C., Schenk, B., van den Berg-Huijsmans, A. A., Koes, B. W., van Buchem, M. A., Arts, M. P., & Peul, W. C. (2015). Percutaneous laser disc decompression versus conventional microdiscectomy in sciatica: a randomized controlled trial. The spine journal : official journal of the North American Spine Society, 15(5), 857–865. doi.org/10.1016/j.spinee.2015.01.020
University of Wisconsin School of Medicine and Public Health. (2021). Home Care Instructions after Lumbar Laminectomy, Decompression or Discectomy Surgery. patient.uwhealth.org/healthfacts/4466